
Overview
The Center seeks to foster and conduct collaborative and transdisciplinary research with global partners through the lens of implementation science, leveraging theories and methods from diverse disciplines to influence migrant health programs and policy.
Sponsored research includes both domestic and international topics through strategic partnering in NYC, NYS and in major immigrant and refugee population centers in the US and abroad.

The Health Equity & Access to Care (HEAC) Project
The HEAC Project is an exciting collaboration with the NYC Department of Health and Mental Hygiene which seeks to better understand New Yorkers’ experiences accessing healthcare in hospitals in New York City (NYC). The goal is to share the results with the health department to inform NYC healthcare recommendations to better serve all New Yorkers.
Gender & Refugee Healthcare
Our newest project, a case study on the intersectionality of gender and refugee status and its effects on healthcare access in Lebanon, is in development in partnership with the Institute for Migration Studies at the Lebanese American University (LAU).

Preliminary Findings from convenings
Convenings with participants from UN Agencies, international humanitarian organizations, health facilities, and local non-government organizations (NGOs) and civil society organizations (CSOs) that work at the intersection of health, refugees and gender were conducted in May 2022. Prominent themes are listed below:
- Lack of registration as potenial vulnerability
- The economic crisis has a similar effect on refugee and host population
- Need for multidisciplinary, intersectional, holistic and inclusive approach and services
- Notable increase in gender-based violence in light of COVID-19
Conservative region in Northern Lebanon and stigma does not allow for open access of services to gender minorities - Main barriers to accessing healthcare: Transportation, cost of fuel, internet connection, lack of privacy, possibility of harassment, retaliation and outing when seeking gender-inclusive services
- Lack of healthcare providers trained in dealing with gender-minority cases and hence lack of gender-inclusive services
Migrant Health CBOs in NY
In January 2021, CIRGH launched a cross-sectional survey of migrant-serving organizations in NYC to collect important information on their early experiences with COVID-19, focusing on the five areas of funding, staff capacity, technological capacity of communities served, resources in communities served, and difficulty working remotely.
Key Study Findings
Organizational capacity is somewhat correlated with number of groups served and types of services offered:
- Smaller organizations tend to offer health and social services, i.e., more day-to-day “survival” assistance
- Larger organizations report greater involvement in areas related to education and employment
- All organizations offer legal assistance
Fear and ineligibility due to legal status are the service barriers cited most frequently
Topics and resources frequently identified for support include: support for advocacy and communications around migrant policy (86%), provision of best practices and policies through a resource hub (55%), access to interns (55%), connections to researchers (50%), and convening spaces (50%)

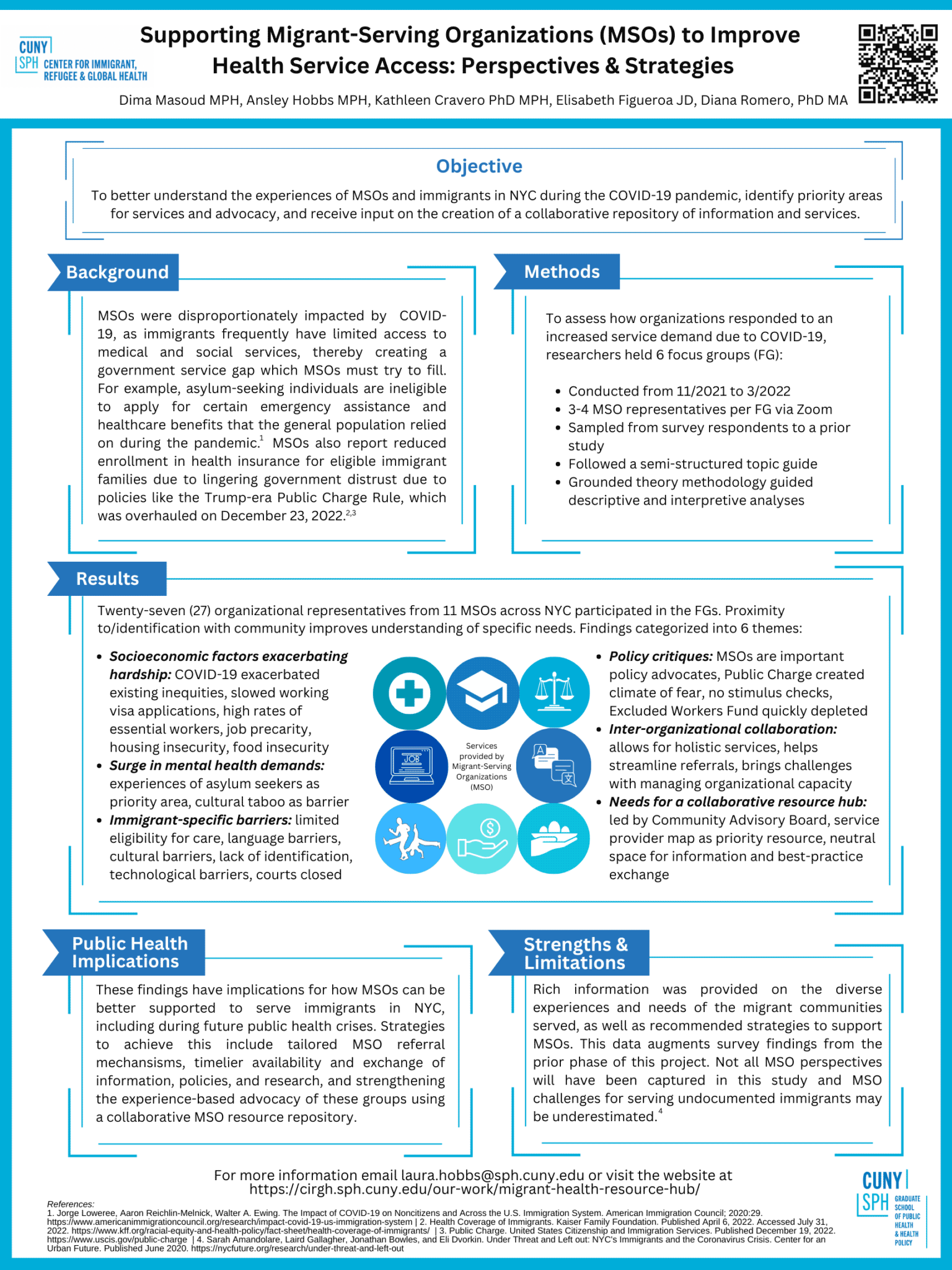
Supporting Migrant-Serving Organizations (MSOs) to Improve Health Service Access: Perspectives & Strategies
Dima Masoud and Ansley Hobbs will represent CIRGH at this year’s North American Refugee Health Conference during the poster session on June 22. Make sure to stop by our poster to learn about the results of the recent focus group study that informed the development of the Migrant Service Provider Resource Center. See you in Calgary!
Supporting Organizations to Improve Migrants’ Access to Health Services in New York City
CIRGH surveyed community-based, migrant-serving organizations (MSOs) in New York City (NYC) regarding their experiences early during the COVID-19 pandemic and perspectives on academic collaborations. Thirty-eight MSOs identified COVID-19-related challenges, including limited staff capacity, organizational funding, and technological and resource limitations of communities served. Organizational capacity correlated with types of services offered. MSOs indicated interest in collaboration on migrant policy advocacy and communications, access to interns, and resources regarding best practices and policies.
Results
Service Provision
The survey found that community-based organizations in NYC fill a critical service gap for immigrants and refugees, with a majority of MSOs surveyed serving multiple populations and offering multiple types of services, including legal assistance, social services, education, health, and employment assistance. Most organizations served undocumented individuals (97.4%), lawful permanent residents (84.2%), and naturalized citizens (78.9%), with fewer services related to student visa holders (34.2%), employment-based visa holders (39.5%), and unaccompanied child migrants (39.5%).

Impact of COVID-19 on Organizational Operations
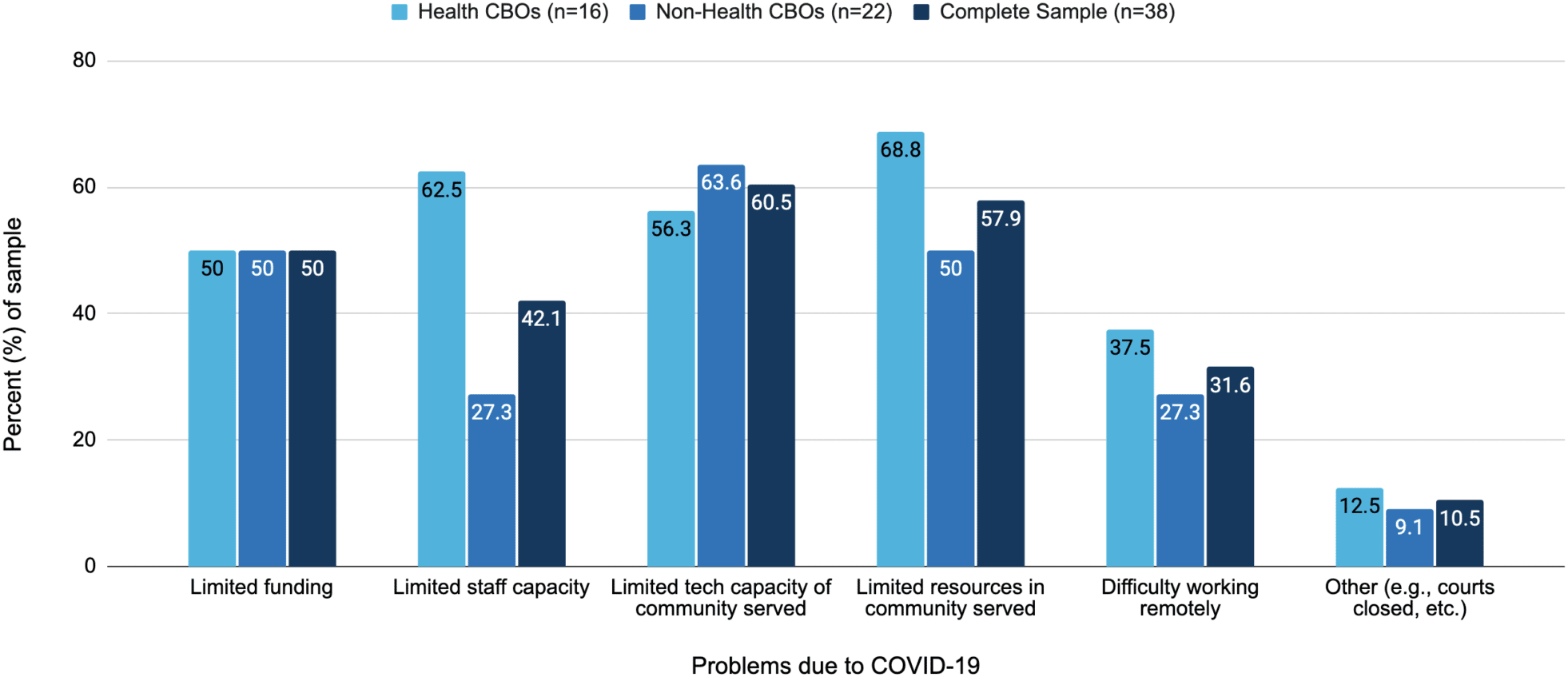
We also assessed the impact of COVID-19 on migrant-serving MSOs, including those with a specific focus on health, regarding limitations in the five areas of funding, staff capacity, technological capacity of communities served, resources in communities served, and difficulty working remotely, as well as other issues reported by respondents. Limited funding was reported by about half of the sample. Health-focused organizations were more likely to report limited staff capacity than non-health organizations (63% vs. 27%), as well as limited resources in communities served (69% vs. 50%) and difficulty working remotely (37% vs. 27%). Limited technological capacity of communities served was reported more by non-health focused organizations (64%) than by health-focused organizations (56%). Other less frequent issues related to COVID-19 were court closures, remote learning, and limited operating space.
Factors facilitating or hindering the access of organization’s clients to programs and services
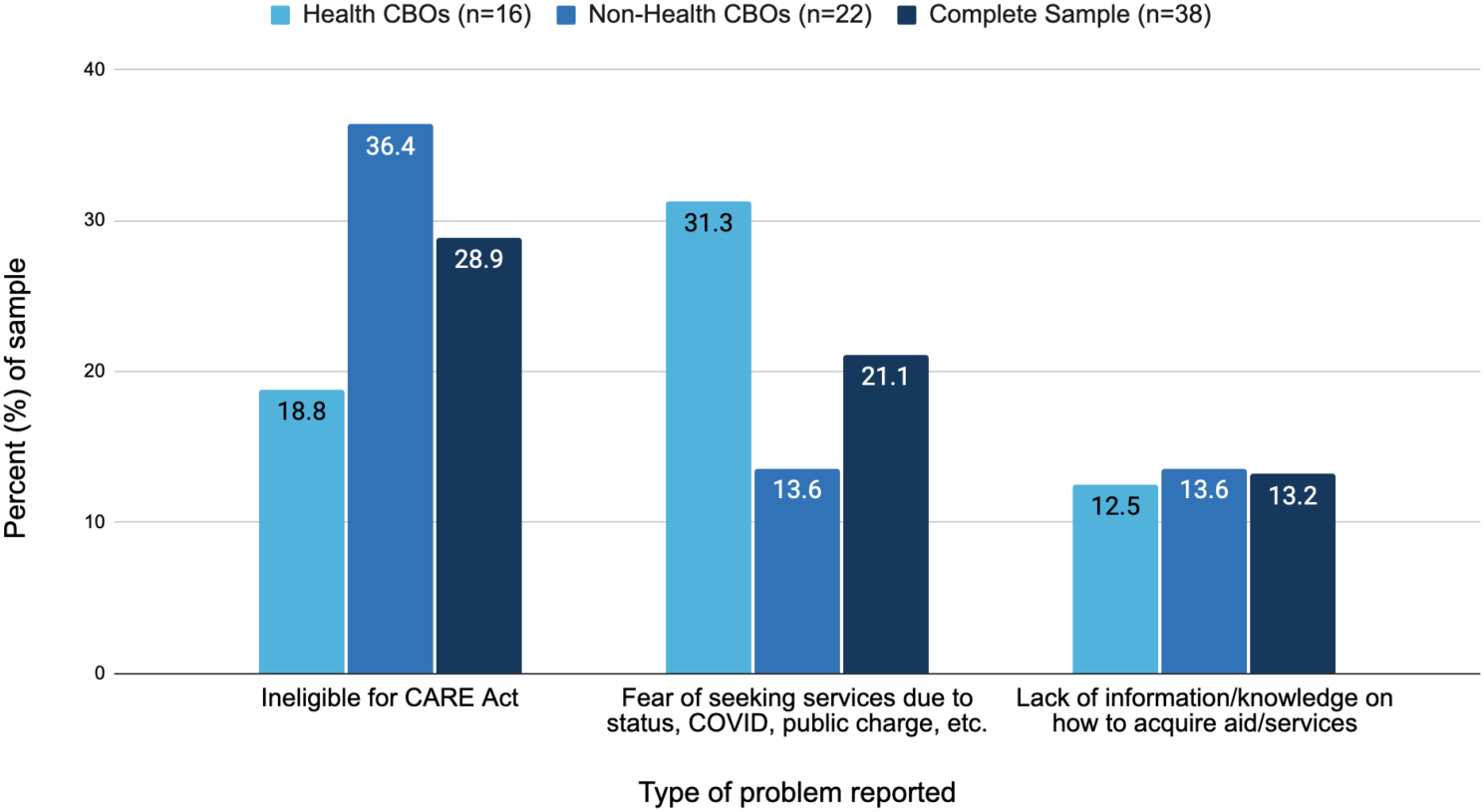
We included an open-ended question on the factors hindering migrant access to programs and services and subjected the responses to word-cloud analysis, which identified the words ineligible, fear, undocumented, and unemployed as the most prominent. Further thematic analysis resulted in three substantive categories: 1) ineligible for CARE Act; 2) fear of seeking services due to migrant status, COVID-19, public charge risk, etc.; and 3) lack of information/knowledge on how to acquire aid and other services. Analysis by organizational type revealed that non-health focused MSOs more often reported ineligibility for the CARE Act as the primary problem affecting their clients compared to health-focused MSOs (36% vs. 19%). Fear of seeking services was reported by 31% of health-focused MSOs, while just 14% of non-health focused MSOs raised the issue. Lack of information/knowledge regarding services was evenly distributed.
Scaling the Effort
The NYC-focused MSO study is being scaled into a statewide intervention in 2022. The decision to broaden the scope of the intervention to the state level is rooted in the understanding that NYC is often just an entry point for migrants, with well over one million immigrants and refugees settled throughout New York State. Some cities like Buffalo have seen population growth—and an increase in federal funding—for the first time in 70 years, in large part due to the arrival of immigrant and refugee communities. Additionally, many of the policies affecting the health of migrants in New York City are designed and implemented at the state-level. Therefore, we want to foster collaboration with and between MSOs and policymakers to ensure new constituents across the state are both considered and included in policy dialogue.
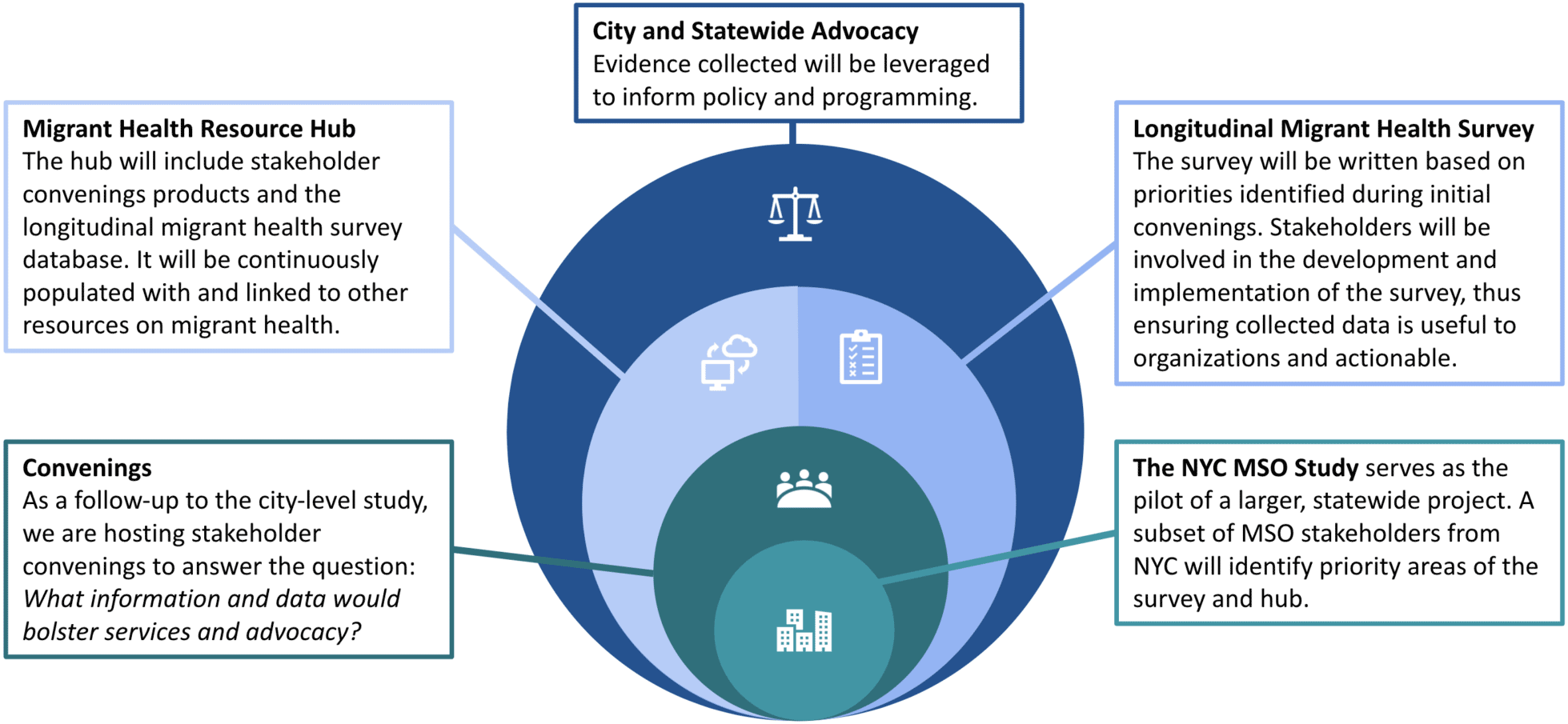
In response to our findings, we are developing the Migrant Health Resource Hub (MHRH). The MHRH addresses the absence of and need for a comprehensive source of NYC/S migrant health data, research and policy information, and serves as a convener to promote statewide multi-sectoral engagement between organizations, policymakers, and researchers. The components described below will advance the activities of the MHRH and build directly on findings from our recent research with MSOs in the context of the COVID-19 pandemic.
The hub will house a migrant health dashboard to visualize and communicate the results of the longitudinal survey, as well as the following stakeholder-identified resources: filterable map and directory of organizations and services (500+ organizations identified), programming toolkits, policy directory and briefs, interpretation and translation services, expert witness testimony services, internship matching, migrant-focused grant postings, training and certificate programs (e.g., Migrant Health Worker training, mental health and psychosocial support trainings via the Mental Health and Psychosocial Support Knowledge Hub, Assistive Technologies with International Society of Wheelchair Professionals, etc.), and pertinent open-source publications.
MSOs and other stakeholders across NYC/S lack a centralized convener and resource for fostering data/information exchange to better serve migrant communities and provide a space for policy dialogue and evidence-informed advocacy planning. The MHRH will sponsor quarterly convenings with stakeholders to advance health policy dialogue between organizations and encourage consistent stakeholder engagement and input.
CIRGH also seeks to promote intentional dialogue between organizations and city- and state-level policymakers. CIRGH and CUNY SPH have existing relationships with policymakers at the NYC Department of Health and Mental Hygiene and the New York State Department of Health, putting us in a unique position to support intersectoral town hall meetings to discuss governmental policy and programming. We currently host digital convening spaces for MSOs and other relevant stakeholders, but there is interest in attending in-person meetings to discuss policy advocacy priorities in 2022.
There is currently no comprehensive, longitudinal data source measuring migrant health in NYC/S. Using MSO/stakeholder input from the convenings, we are co-developing a survey to regularly assess the health of migrants across the state. Rooted in data equity, the longitudinal survey is being developed with the input of organizational and community stakeholders to determine what data are collected, how the data will be used, and how migrant experiences are captured.
The database will allow for monitoring migrant health over time and across New York’s ten geographic regions: Capital District, Central New York, Finger Lakes, Mid-Hudson, Long Island, Mohawk Valley, New York City, North Country, Southern Tier, and Western New York.
